Esophageal Foreign Bodies
The definitive treatment for removal is endoscopy with direct visualization and removal of the object causing the obstruction. This procedure is invasive, time consuming, requires a gastroenterologist, as well as procedural sedation. Due to the time it takes to set up for this procedure, many consultants will ask to try medical therapy first - Salim Rezaie
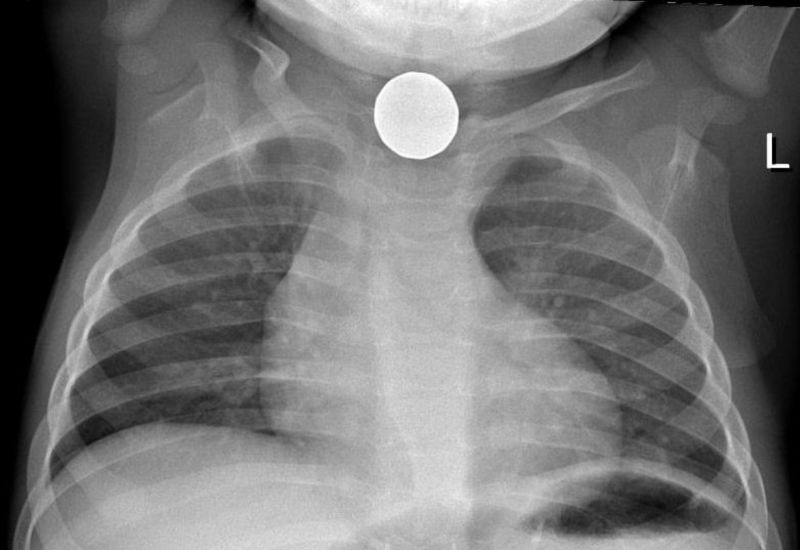
image by: Samir
HWN Suggests
The ‘Olden Days’ and the (o)esophagus
But, I was surprised that the only recommended medical management was IV glucagon. I gave up on that decades ago – it’s never worked for me (except when the patient vomits from the glucagon, and blasts the food bolus out through his eyeballs – if you try this stuff, give it really slow), and in studies, it seems to generally be outperformed by placebo.
Somewhere back in the early 70’s, I learned – and I don’t recall from whom or where – that GTN (glyceryl trinitrite, or NTG aka nitroglycerin for those in the upper half of the globe) worked well for lower esophageal food impactions.
Resources
 Sirens to Scrubs: Esophageal Foreign Body Obstructions
Sirens to Scrubs: Esophageal Foreign Body Obstructions
It’s easy for us to describe esophageal FBOs when it is a clear-cut presentation, but it can actually be challenging to distinguish between esophageal and airway FBOs, especially in children. Always be suspicious that this may be choking directly due to airway obstruction.
Question Tradition: Glucagon for Food Boluses
Esophageal foreign body impactions are a rare entity, that cause quite a bit of discomfort to patients and have the potential for esophageal necrosis and perforation. The definitive treatment for removal is endoscopy with direct visualization and removal of the object causing the obstruction. This procedure is invasive, time consuming, requires a gastroenterologist, as well as procedural sedation. Due to the time it takes to set up for this procedure, many consultants will ask to try medical therapy first.
Stuck in the Middle with Food...
Esophageal foreign body impaction (EFBI) is the most common foreign body impaction seen in emergency departments in the United States and accounts for about 75% of cases. Although estimates vary, the majority of foreign body impactions are meat boluses. In addition, the clinical presentation of these cases is complicated by the presence of baseline esophageal pathology, ranging anywhere from 30 to 90%
Bougienage for Esophageal Foreign Bodies in Children
One condition that we often don’t consider, but perhaps we should more, is a stuck Esophageal Foreign Body (FB). Let us review how we can become Superheroes in this realm as well – Bougienage for Esophageal Foreign Bodies in Children...
Bougienage Good Alternative for Treating Retained Esophageal Coins
Bougienage has been around for decades, but it remains an infrequently used modality for the treatment of retained esophageal coins. While the feared button-battery ingestion can cause esophageal necrosis in as little as two hours, impacted coins can also cause perforation, obstruction, or fistulas if left untreated.
EM@3AM: Esophageal Foreign Bodies
Glucagon 1-2 mg IV or IM may relax the lower esophageal sphincter. Data are controversial regarding efficacy. Major side effect is nausea and vomiting, which increases risk of tissue damage. Provide antiemetic before glucagon is given (such as ondansetron). Carbonated beverages may result in dilation of the esophagus, though data are controversial. Other medications (nifedipine, benzodiazepines, nitroglycerin, papain) have low success rate and risk of side effects. They are not recommended for use.
Endoscopic removal of foreign bodies from the upper gastrointestinal tract: 5-year experience
Esophagus was the most common site of trapping (27/45); FBs were trapped in both upper (the narrowest site) and lower (the commonest site of stricture) parts of the esophagus.
Esophageal Foreign Bodies
The indication for pharmacologic relaxation of the LES is the presence of a smooth or blunt FB such as a coin or food bolus. Angulated, abrasive, or sharp FBs should not be treated with pharmacologic modalities but instead should be removed by esophagoscopy. Analgesics and sedatives are routinely indicated if pain is present or the patient is excessively anxious.
Impacted Pills
Before we entertained the pharmacologic options, we gave the patient a can of Ensure, because it has a higher viscosity than water. Fifteen minutes later, the pill was pushed into the stomach and the patient’s foreign-body symptoms resolved. A simple $1.50 solution.
Non-traumatic Foreign Bodies of the HEENT and Esophagus
In general, any pediatric foreign body in the esophagus is considered impacted and requires removal as soon as possible.
The ‘Olden Days’ and the (o)esophagus
Most patients are able to point to the level of impaction – base of the neck for cricopharyngeus muscle level of obstruction, lower sternum for obstruction at the lower esophageal sphincter. One would expect GTN to work at the LES but not at the cricopharyngeus – smooth muscle vs striated muscle, and all that – and that has been true in my experience. I suppose that a trial of a benzo might work at the cricopharyngeus, but I can’t recall having done that.
StatPearls
The most common complication seen is impaction, which is most frequently within the esophagus. There are three sections of the esophagus where foreign bodies are at higher risk of becoming impacted due to narrowing. First, and most commonly, is at the thoracic inlet where the cricopharyngeus muscle is located. The second section is at the aortic arch, and the third section is at the gastroesophageal junction.

Introducing Stitches!
Your Path to Meaningful Connections in the World of Health and Medicine
Connect, Collaborate, and Engage!
Coming Soon - Stitches, the innovative chat app from the creators of HWN. Join meaningful conversations on health and medical topics. Share text, images, and videos seamlessly. Connect directly within HWN's topic pages and articles.












