Shock
Regardless of the underlying cause, all forms of shock share a common concern: inadequate perfusion - Garret E. Pachtinger
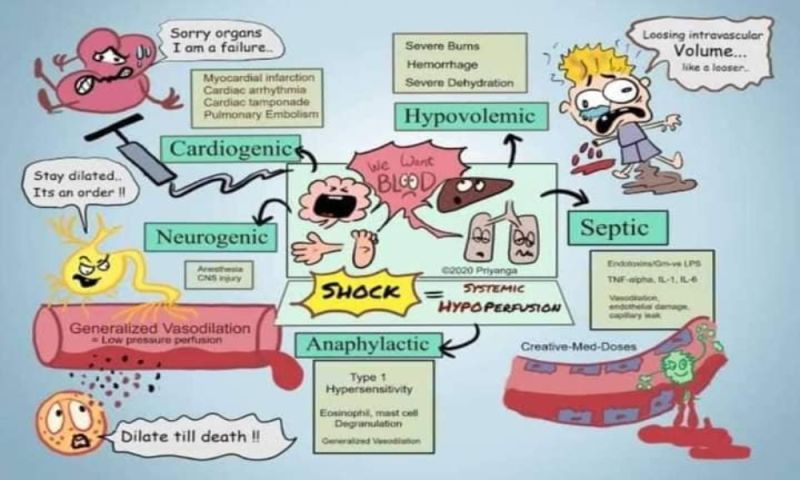
image by: Pejumedical blog
HWN Suggests
Shock… Do We Know It When We See It?
Our curious and short human history is littered with betrayals.
We betray each other with alarming regularity – Judas Iscariot, Marcus Brutus, Benedict Arnold and Tokyo Rose are all part of our collective history, and, if not salient, at least provide insightful looks at our relationships.
But, like the portly naked Emperor, we also betray ourselves, based on falsehoods and groupthink, parading with certainty through the town, convinced of our correctness. Medicine can sometimes be like this, with countless examples of teachings, tools, guidelines and texts that do not always have truth at their heart.
Once in a while, it’s worth examining the truths we think…
Resources
 Big Shock…..Do we ❤ POCUS?
Big Shock…..Do we ❤ POCUS?
Although the evidence for POCUS in shocked patients doesn’t show a survival benefit it does support the view that it is a useful adjunct for clinicians in diagnosing and treating patients.
An approach to undifferentiated hypotension
If there is an obvious cause of the hypotension, such as trauma or a GI bleed, you don’t need this approach. Just start treatment as usual. Control the airway and supply oxygen. Most times this will be with basic airways maneuvers or an LMA. You can always intubate later when you have the patient better resuscitated.
Approach to the Critically Ill Child: Shock
To understand how kids with shock present differently than adults, it’s important to discuss a few basic differences regarding intravascular volume and cardiovascular system in children especially neonates and infants (1-24 months of age). Also remember shock is defined the exact same way as it would be in adults even though the presentation and underlying physiology may differ. Shock is simply a state where tissue/organ blood flow is inadequate to meet tissue/organ metabolic demands.
Resus of the hypotensive patient Part 1 - When IV Fluids Kill
There is probably no other drug emergency providers administer more often than IV fluids. We give them to patients with mild heat exhaustion, gastroenteritis and orthostatic dizziness to name a few. These patients tend to feel better, go home and no harm comes to them. However, for the subset of patients with shock and potential recipients of large volume resuscitation, excessive IV fluids can harm.
Approach to shock
Shock is a state of systemic hypoperfusion, with inadequate blood supply to the tissues. Unfortunately, this may occur in different ways. The most simple physiology of shock is cardiogenic shock, with low cardiac output to the entire body. However, septic shock can occur with an elevated cardiac output due to microvascular dysfunction at the tissue level (blood shunts through some vessels, while ignoring others). Because shock has varying physiologies, it defies any simple operational definition at the clinical level. Shock is a bit like obscenity – after a while, you know it when you see it.
EM in 5: Shock
To better understand and manage patients in shock, we can think about splitting them into 4 categories: Hypovolemic, Cardiogenic, Distributive, Obstructive.
The general approach to the patient in shock
"Permissive hypotension" in trauma: Principle that guides the fluid resuscitation of traumatic patients who arrive hypotensive to stay somewhat hypotensive until blood loss is source-controlled.
RUSH (“Rapid Ultrasound for Shock”) Protocol
One of multiple described ultrasound protocols for evaluation of patients presenting to ED with undifferentiated hypotension. Provides a framework for rapid and systematic evaluation of cause of hypotension •Three categories •Pump – Cardiac evaluation •Tank – Volume status •Pipes – Vascular system •Equipment: Ultrasound machine with phased array (3.5-5MHz) and linear probes (7.5 – 10MHz).
Albumin versus normal saline
Crystalloid vs colloid - no clear advantage of either
Some Miscellaneous Tidbits About Shock
The abnormally low cardiac output that we term "shock" can result from several causes. Understanding how shock can develop and how the cardiovascular system's regulatory mechanisms respond is interesting in its own right, and it also provides some useful insights into the normal functioning of the regulatory mechanisms...
Choosing the right vasopressor agent in hypotension
Persistent hypotension results in impaired tissue perfusion and is often a late and ominous indication of decompensated shock. Correction of persistent hypotension is imperative, often requiring vasopressors and inotropes. When considering an agent for hemodynamic support, the following checklist can guide your choice...
Colloids vs. Crystalloids for Critically Ill Patients Presenting with Hypovolemic Shock
In ICU patients with hypovolemia requiring resuscitation, the use of colloids vs. crystalloids did not result in a significant difference in 28-day mortality; however, 90-day mortality was lower among patients receiving colloids.
Do colloids save lives in hypovolemic shock?
So, your patient's in shock: quick, give some fluids. But colloids or crystalloids? How to choose? They both raise blood pressure, they both improve organ perfusion -- but one's less filling, the other tastes great (what, you haven't tried them?).
Resuscitation Fluids
Fluid resuscitation with colloid and crystalloid solutions is a ubiquitous intervention in acute medicine. The selection and use of resuscitation fluids is based on physiological principles, but clinical practice is determined largely by clinician preference, with marked regional variation. No ideal resuscitation fluid exists. There is emerging evidence that the type and dose of resuscitation fluid may affect patient-centered outcomes.
Shock
At the cellular level, shock hypoxemia causes cell membrane dysfunction leading to intracellular edema and leakage, as well inability to regulate cellular pH. This causes progressive acidemia, which in turn, have severe systemic effects on multiple organ systems.
Shock Review: Goals of Therapy
While simple in theory, the complexity of the body's response to shock and its therapies can make realtime goal-directed management of shock surprisingly challenging.
Shock Review: Mechanisms and Therapies
Need a mnemonic? Authors propose "VIP": Ventilation (oxygen, intubation etc), Infusion (volume resuscitation), Pump (vasoactive drugs) to manage people in shock.
The Ongoing Controversy: Crystalloids Versus Colloids
There is still much debate over the optimal fluid to use for resuscitation. Different studies have indicated either crystalloid or colloid is the ideal intravenous solution to administer, based on mortality or various physiological parameters. Older studies found differences between crystalloids and colloids. However, with the evolving science of fluid administration, more recent studies have shown no differences in patient outcomes.
Shock… Do We Know It When We See It?
Our curious and short human history is littered with betrayals. We betray each other with alarming regularity – Judas Iscariot, Marcus Brutus, Benedict Arnold and Tokyo Rose are all part of our collective history, and, if not salient, at least provide insightful looks at our relationships.
Anaphylaxis and Anaphylactic Shock
All patients who fulfill the criteria for anaphylaxis require the administration of epinephrine. Epinephrine is the only drug to show a mortality benefit in the management of anaphylaxis.
Cardiogenic Shock
Tissue hypoperfusion that is primarily attributable to damage to the heart.
Circulatory Shock
Shock is the clinical expression of circulatory failure that results in inadequate cellular oxygen utilization. Shock is a common condition in critical care, affecting about one third of patients in the intensive care unit.
Hemorrhagic Shock
Blood products need to be available in the trauma bay for when these patients arrive. If you need to give crystalloid while awaiting the products, give only small amounts just to keep the patients heart beating.
Neurogenic Shock
Even when the mechanism is highly suggestive for significant spinal injury, the shocked major trauma patient is haemorrhaging until proven otherwise; cue blood products and damage control resuscitation. When there is no evidence of external haemorrhage in the primary survey, the EFAST is negative, and the trauma series CT shows no evidence of bleeding, a diagnosis of neurogenic shock can be considered, particularly if there is obvious focal neurological deficit.
Pediatric Sepsis and Septic Shock
Kids aren’t little adults. Pediatric sepsis and septic shock usually presents as ‘cold shock’ where as adult septic shock usually presents as ‘warm shock’, for example.
Septic shock: Rapid recognition and initial resuscitation in children
The use of colloid for fluid resuscitation for children with septic shock is controversial. Nevertheless, colloid infusion with albumin 5 percent is a reasonable option for children who have not improved following >60 mL/kg of crystalloid fluid, have hypoalbuminemia (albumin <3 g/dL), or who develop a hyperchloremic metabolic acidosis.
SIRS, Sepsis, and Septic Shock Criteria
•When a patient presents with two or more SIRS criteria but with hemodynamic stability (i.e. blood pressure at baseline), a clinical assessment must be made to determine the possibility of an infectious etiology.
Spinal Shock
Spinal shock is not really "shock" in the sense of circulatory collapse but rather a transient or temporary (physiologic rather than anatomical) complete loss of all neurologic function, including reflexes and rectal tone, below a specific level that is associated with autonomic dysfunction. This phenomenon was first described in 1750 by Whytt.
Trauma Resuscitation
Shock is defined as inadequate delivery of oxygen to the tissues. Therefore our goal in the treatment of shock is to improve oxygen delivery.
#Rush
Treatment depends on the cause of hypoperfusion. PUMP problem? Maybe you need an inotrope or other cardiac support TANK problem? Then fill up the tank. Use whatever fluid you need, but remember crystalloid doesn’t carry oxygen. PIPE problem? Then, assuming you have a full tank, you need a pressor.
PedsCases
The many causes for shock are generally subclassified as hypovolemic, cardiogenic, septic and distributive or neurogenic shock. Let’s talk about each of these in detail.

Introducing Stitches!
Your Path to Meaningful Connections in the World of Health and Medicine
Connect, Collaborate, and Engage!
Coming Soon - Stitches, the innovative chat app from the creators of HWN. Join meaningful conversations on health and medical topics. Share text, images, and videos seamlessly. Connect directly within HWN's topic pages and articles.












